
Why The United States Health Care System Costs So Much – Part Five – Prices
OK, folks, this is where the money is. Yes, this is the absolute crux of why our health care costs so much.
When I was working in physician groups who were capitated (paid a set amount of dollars per patient per month) instead of fee-for-service (paid a set amount for each service provided) the number one thing the physician groups did was negotiate the lowest prices or figured out a way to pay less for something. That’s because the physician groups had to pay the other “external to themselves” health care providers from that capitation payment. They combined being efficient within their offices and practicing evidence-based medicine (aligned with best practices) with getting the lowest prices.
When I was in hospital system based health care systems, this was not the case. During those times, I was the Chief Medical Officer of the hospital systems’ health insurance plans. Because a hospital system’s mentality is to make as much operating/profit margin as possible, trying to be the lowest cost service provider in the market wasn’t in their DNA. This was especially true for the Finance folks. They are laser focused on decreasing utilization…for all the other service providers, not necessarily their hospital-based system, not lowering their prices. I once convinced the administration to apply a lower fee schedule for a health plan account for the hospital system’s services to retain the account and the Finance guy looked like you had stabbed him in the heart, that’s how hard it is for them to lower prices.
I used to have quarterly reports showing utilization flat or decreasing in 90% of the service providers while prices were consistently increasing and the finance folks demanded further reductions in utilization rates to offset the price increases because they had no appetite to try to decrease prices.
Hospitals can be very creative in maintaining their prices. You’ve probably read news articles about hospital “chargemasters” which have absolutely no basis in any type of business logic except the hospital system is operating in the USA free market system. So, their chargemasters look a lot like the Drug Company way of pricing things, that is, charging whatever they think the market can bear. I’ve watched this in action, even in IDS’s that, to the public, voice that they want to be the most affordable health care system. But that is actually a huge lie.
But don’t take my word for it. Read this article: US Hospitals Are Still Using Chargemaster Markups To Maximize Revenues, by Ge Bai, and Gerard F. Anderson. Here’s an excerpt:
“Using 2013 nationally representative hospital data from Medicare, we found that a one-unit increase in the charge-to-cost ratio (chargemaster price divided by Medicare-allowable cost) was associated with $64 higher patient care revenue per adjusted discharge. Furthermore, hospitals appeared to systematically adjust their charge-to-cost ratios: The average ratio ranged between 1.8 and 28.5 across patient care departments, and for-profit hospitals were associated with a 2.30 and a 2.07 higher charge-to-cost ratio than government and nonprofit hospitals, respectively.”
“These findings suggest that hospitals still consider the chargemaster price to be an important way to enhance revenue.”
The statement “The average ratio ranged between 1.8 and 28.5 across patient care departments” means the hospital chargemaster is setting prices almost 30 times the Medicare allowable reimbursement for some services!!
If you don’t have insurance, the chargemaster prices are what the hospital will charge you. I usually told uninsured patients who really needed the hospital care to start negotiations with the hospital at 1/3 of whatever the hospital billing folks told them they owed the hospital.
In one state in which I worked, the reimbursement model was a DRG (Diagnosis Related Group, a payment type started by Medicare. It is a “lump sum” payment for an admission rather than a line by line item charged) model. But, when the charges (not network fee-for-service equivalents) for the line items for an admission reached a certain dollar amount (let’s say $30,000), the reimbursement to the hospital reverted to a percent (like 80%) of billed charges. Now that you know how perverse the hospital chargemaster system is. This makes no business sense for the person or entity having to pay the bill. Even though the Finance and administration folks knew this was creating excessive prices for admissions, they wouldn’t change their own DRG model to mimic Medicare (which doesn’t do this at all) for their own health plan because they wanted to maintain that perverse DRG model with the other health plans and health insurance companies, obviously, because it was more lucrative. Yes, maintain as high of prices as possible. Not surprising. And, since a hospital can raise the charges in a chargemaster anytime they want, if they need more cash, they just raise the chargemaster prices.
Yes, just like the Pharmaceutical companies raise drug process whenever they want. Since the hospitals are getting 80% of charges when they hit the DRG related “charges dollar amount”, the higher the charges, the more cash! And no one can stop them.
[Factoid: You should never negotiate a contract with a health care service provider based on a percent of their charges. You need to define a fee schedule. Otherwise you are at the mercy of the health care providers’ whimsical self-benefitting alterations in their charges.]
The main reason for this is, it helped the hospital system’s profit margin to maintain prices. As a matter of fact, it was common that the highest priced service providers in a hospital system owned health plan network were….wait for it….providers owned by the parent hospital system! Who would have thunk…NOT!! This shuttles money from the health plan to the “delivery system” to maximize the financial health of the hospital system. The health plan was supposed to make up for this loss to their bottom line by ratcheting down on utilization of services by non-hospital system service providers. This is why the Finance folks in Integrated Delivery System’s (this is when a hospital system owns a lot of the health care delivery and financing (insurance) businesses, including doctors) are stuck on utilization decreases of other health care providers vs. becoming more efficient or reducing the margin on their services to make health care more affordable. Greedy, greedy greedy.
And there seemed to be this phenomenon that the hospital system and all the other providers were in the same buddy-buddy situation, meaning, it was hard for them to drive down other service provider prices because they inherently didn’t want that done to themselves. It was sort of like doctors don’t like to say an averse outcome has any doctor culpability because of the “that could have been me” mentality (you have no idea how many times I heard that in Quality Case Review sessions).
Here’s another hospital price maximization tactic.
The Facility Fee.
In 2000, Medicare created the facility fee. They set new billing standards for employed physicians. Some say it was meant for teaching hospitals (who always seem to need more money) who had their attending physician offices attached or integrated into the teaching hospitals on the same campus. However, this wasn’t specified in the new rule.
As with other billing standards, commercial health insurers simply adopted what Medicare does. So, non-teaching hospitals, reviewing the specifications of the new rules, realized that if they declared their hospital-owned physician group offices as a department of the hospital, they, too could charge the facility fee. Most of these offices are free-standing offices, just like an independent physician’s office. Of course, the hospitals say they need the facility fee to maintain these offices, but, that’s just how they justify charging the fee. It’s not true. The private physician doesn’t need this.
What a facility fee does is dramatically increase the cost for a physician office visit or any test that is done in a hospital-owned physician office.
Here’s a couple of examples:
In 2012 and 2014, the Medicare Payment Advisory Commission analyzed Medicare data. According to the 2014 report, Medicare, for echocardiograms (ultrasound of the heart) paid, on average, $453 at a hospital-owned facility and $189 at a privately-owned office. Keep in mind that providers are paid by a Medicare fee schedule, not based on a percent of charges. This means that the Medicare “payment standards” allowed a 2.4 times increase in payment for the same service! According to the 2012 report, they paid $124.40 for a 15 minute office visit at a hospital owned physician office and $68.97 at a privately-owned physician office, almost twice as much!
There is a facility fee for just about everything. This became a cash cow for hospitals. So, they started employing physicians to expand their ability to receive this extra cash. I’m here to tell you that running a physician office costs the same whether a hospital owns it or not. I actually had a hospital take over my practice in the 1980’s. Nothing in the office changes, same staff, same supplies, etc. So, if it were 2001 instead of 1989, the prices for my services would have doubled overnight with no increase in costs to run the practice. This happens all the time now.
What this means is WE ARE ALL PAYING FOR THIS! If you are in a high deductible health plan, are uninsured or on Original Medicare (where you pay 20% of what Medicare pays a doctor), your out of pocket costs are higher. For those on a copay plan, your insurance premium is higher and, no matter which plan you are in, your taxes are higher (because YOU have to pay the taxes to pay for the 80% Medicare pays which includes this facility fee charge).
President Obama signed a bill that, going forward, only allows for facility fee payment if the physician office is on the same campus as the hospitals. But, it “grandfathers” the physician offices or other service facilities already owned by hospitals that are not on the same campus starting 2018!. ALERT: Watch for your local hospital to start building facilities on their hospital campuses and move their employed physicians to the campus!
The 2014 report says Medicare would save about $500 million if they stopped paying facility fees for physician offices.
My personal opinion is, no physician office should be able to charge a facility fee. It’s perverse.
For hospitals, in addition to using every method possible to maximize their revenue, they are consolidating. Consolidation creates, at the least, a near monopoly within a region so that the hospitals can demand higher prices for the services they own.
But don’t take my word for it:
As Hospital Chains Grow, So Do Their Prices For Care, By Chad Terhune June 13, 2016 Kaiser Health News. Here’s an excerpt:
“As health care consolidation accelerates nationwide, a new study shows that hospital prices in two of California’s largest health systems were 25 percent higher than at other hospitals around the state.
Researchers said this gap of nearly $4,000 per patient admission was not due to regional wage differences or hospitals treating sicker patients. Rather, they said California’s two biggest hospital chains, Dignity Health and Sutter Health, had used their market power to win higher rates.”
Here’s the actual study: Hospital Prices Increase in California, Especially Among Hospitals in the Largest Multi-hospital Systems, Glenn A. Melnick, PhD and Katya Fonkych, PhD. Here’s an excerpt from the abstract:
“Our data show that hospital prices in California grew substantially (+76% per hospital admission) across all hospitals and all services between 2004 and 2013 and that prices at hospitals that are members of the largest, multi-hospital systems grew substantially more (113%) than prices paid to all other California hospitals (70%). Prices were similar in both groups at the start of the period (approximately $9200 per admission). By the end of the period, prices at hospitals in the largest systems exceeded prices at other California hospitals by almost $4000 per patient admission.”
Inflation has only been running between 1-2% a year, so you do the math as to how ridiculous these price increases are.
I’m here to tell you that this is going on all over the USA. And not just with hospitals. Here’s a doctor one. Variation in Emergency Department vs Internal Medicine Excess Charges in the United States, TimXu, MD, MPP, et al, JAMA Internal Medicine, 2017. Here’s an excerpt:
“Our analysis included 12,337 emergency medicine physicians from 2707 hospitals and 57,607 internal medicine physicians from 3669 hospitals in all 50 states. Services provided by emergency medicine physicians had an overall markup ratio of 4.4 (340% excess charges), which was greater than the markup ratio of 2.1 (110% excess charges) for all services performed by internal medicine physicians [for the same services]”
Of course, the ED physicians work…IN HOSPITALS!! It’s not a leap to figure out they ED docs’ finance guys are talking to the hospital finance guys, now is it?
And then there are the doctors who are in a monopoly or near monopoly position within a city or region. If they are in a market where the doctor group is the only group in that specialty, like Oncologic Surgery or In Vitro Fertilization, or, the doctors are the only PCPs in a rural area, they either won’t contract with a health plan (this means you pay whatever they charge (often 2-3 times what Medicare pays) as a health plan or patient) or they have a contract with the prices they demand (often as high as 3-5 times what Medicare pays). This also applies to any health care service provider (hospitals, Physical therapy, Durable Medical Equipment providers, etc.).
I’ve actually seen illegal activity on the part of doctors trying to get as much money as possible from health plans. In one city there were five solo practitioners in a certain specialty. According to federal law, these five solo practitioners couldn’t negotiate as a unit unless they shared business or clinical systems, which they didn’t. As we tried negotiating with one, that one solo practitioner would pass notes to the other four in the physicians lounge in the hospital so they all would be asking for the same thing or holding out signing contracts until they all maximized their fee schedule at the same price point. At one point another group of solo practitioners came forward as a group, even hiring a lawyer who thought this wasn’t illegal and tried to openly negotiate for them as a unit. They had absolutely no business or clinical integration! Because the health plan was owned by a hospital system, the hospital system told the health plan to capitulate to the doctors and the legal department wouldn’t report them to the Feds (See the above paragraph about the “buddy-buddy” mentality).
I could go one for pages about how all the other service providers I’ve negotiated contracts with are doing the same things, but it would be dozens of boring pages that you wouldn’t read.
The bottom line is, in the USA, health care providers are constantly trying everything they can to get the highest amount of money for their services. You’ve already read and heard about the Pharmaceutical Industry, which has gone totally hog wild with price raising! Now you’ve heard Hospital stories about them doing the same thing!
This is because the Health Care Industry is operating within the rules of a free market system. It’s supposed to be competition driven, but you can see how that competition part doesn’t seem to operate in the health care sector. But the “get as much money as you can get” is still very operative.
All of this results in the USA being the highest cost system in the world without having the best health care outcomes.
Sticking with the Pharmaceutical Industry, my personal favorite target, here are a couple of stories illustrating how this plays out:
Example #1, Getting a drug in another country. I won’t mention the country, but, I’ve done this in three and it was practically identical. There is a drug that treats cold sores called acyclovir. You can get it as a tablet. You can also get it as a cream or ointment. If you have the cream or ointment, you can carry that in your purse or briefcase or have it in a drawer in your office and thereby start it immediately, which hastens the resolution of the cold sore attack, and you don’t have to call your physician or go to Urgent Care to get pills.
Here are some screen shots:
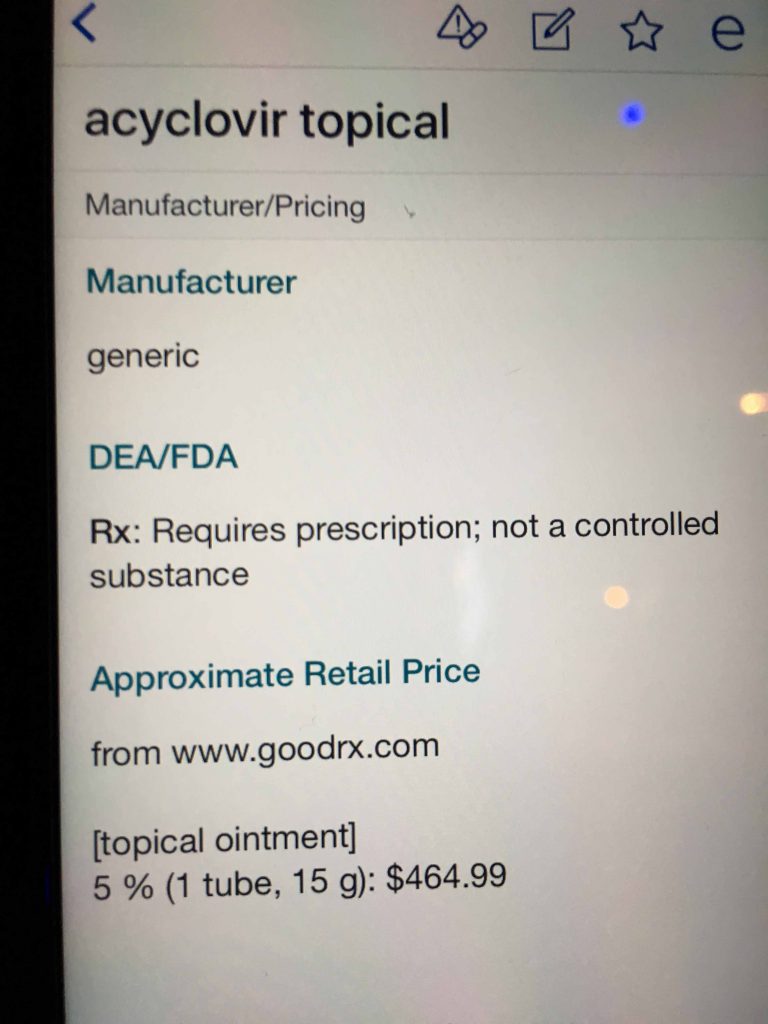
Notice the approximate retail price, $464.99. For a GENERIC! I’m here to tell you that 5 years ago that was about $60.00. Now, the pharmaceutical companies will tell you no one pays the retail price; that this is sort of like the hospital chargemaster. Actually, it sort of is, but, if you don’t have insurance or have access to a coupon program, the retail price is what you will pay.
So, let’s look at the coupon program. This is a screen shot for the same medicine from GoodRx, a popular coupon program:
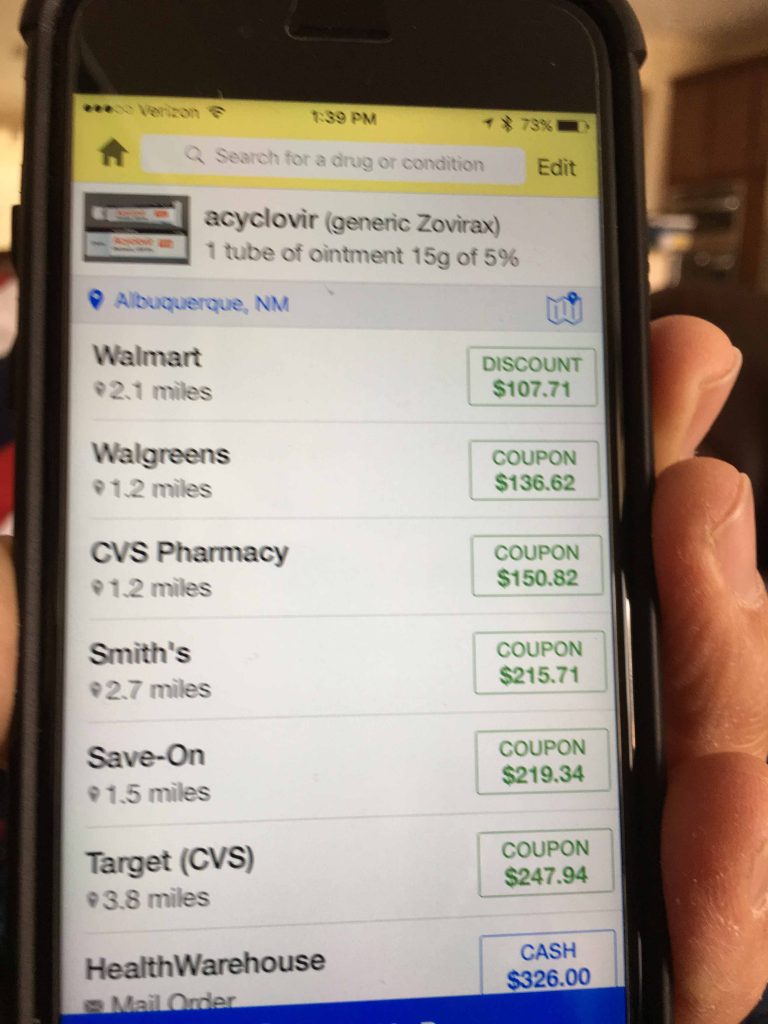
Even with the coupon, this generic medicine is still pricey, and you can pay up to $326.00 for a 15 gram tube. I’m sure this is on everyone’s health plan fourth tier copay, which can be in the $100 range or, if you’re on a high deductible plan, you’re going to pay at the least a price at or above the above Walmart price.
So, here is the actual charge ticket from buying the medicine in another country (the price was within $1.00 among the three countries where I bought this):
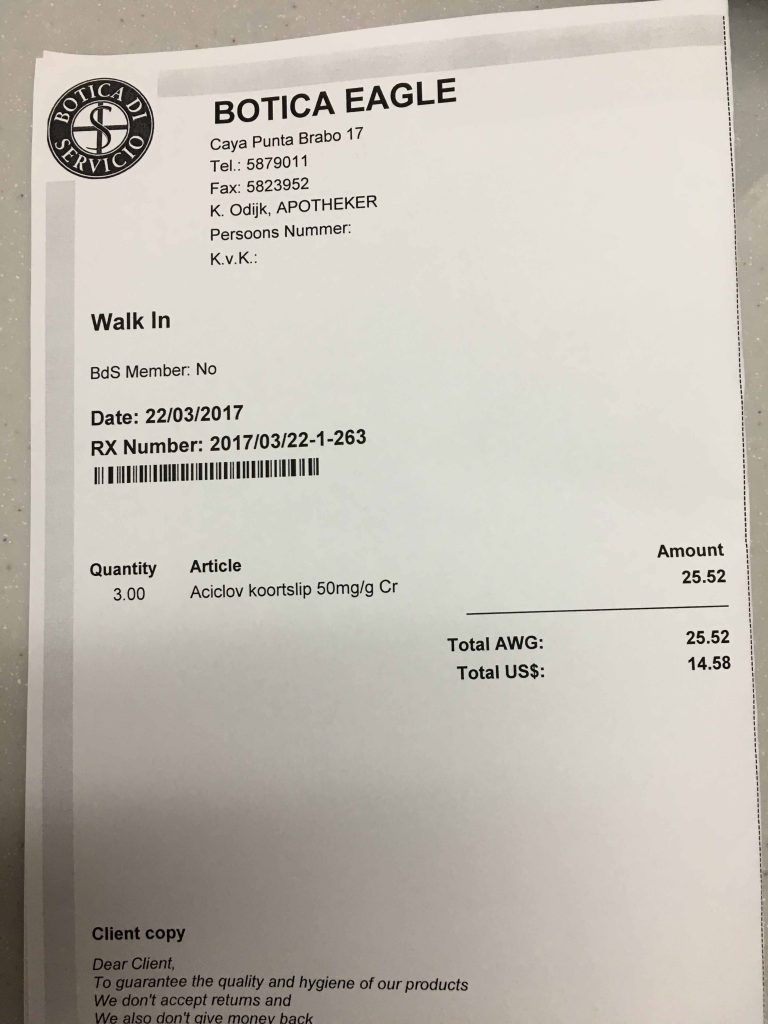
Yes, you are reading that right, $14.58 USD for three 5g tubes (same amount as the one 15g tube in the USA examples)! Thirty-two times less expensive than the USA retail price and 7.4 times less expensive than the cheapest price on GoodRx!!
Here’s another. I’m a senior citizen, so I’m on Medicare and I chose a Medicare Advantage plan. It does have some advantages. At the same time, it has a fourth tier copay for “expensive” drugs. It’s a $95 copay. There is a topical steroid that has been generic for about 30 years, but, because of Pharma operating in a free market society, even the generic for this drug is expensive. Here’s a screen shot:
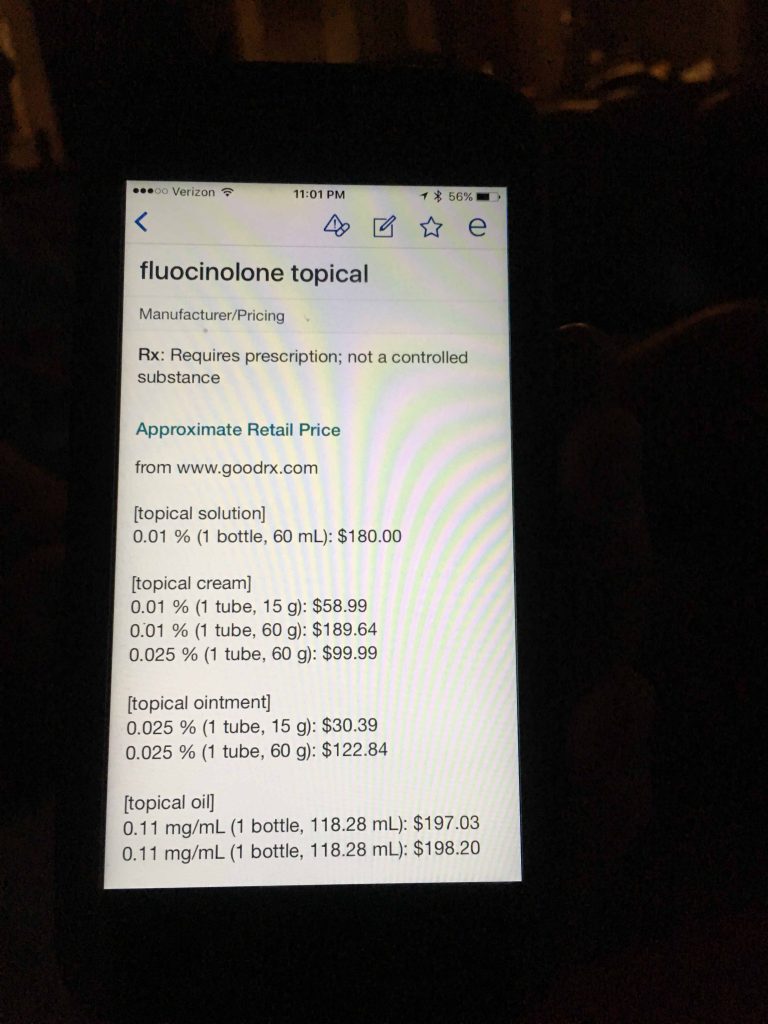
Two ounces of this drug is $180.00! $90 an ounce!
Here’s the GoodRx coupon prices:
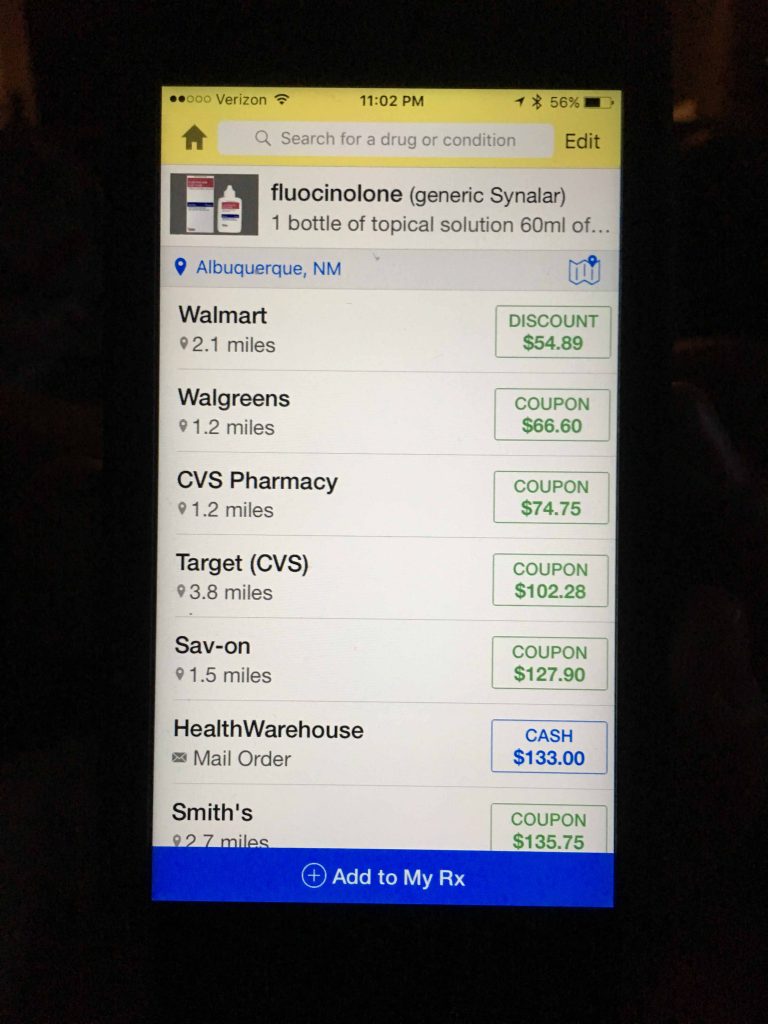
Remember, I paid $95. Three of the stores charge less than $95. If you don’t have a coupon app like GoodRx, go to the app store, get it, and always check the coupon prices against your copay/coinsurance cost. The fact that three stores can offer the drug for less than my copay, I’m wondering if the health plan actually made money from me since my copay is higher than the potential actual cost to the health plan! At the same time, this generic drug is still pretty expensive!
OK, it’s those big bad hospital systems and the drug companies, right? Well, not so fast. It’s also everyone, me included, who work in the health care industry, because we all expect a certain amount of money to do what we do. From doctors to nurses to physical therapists to pharmacists (you name it, even chiropractors), we are accustomed to getting paid darn well. And actually, it’s a lot more than other countries. But, then again, we’re in a free market society, so, we’ll take whatever the market can bear! I’ll show you this in some graphs later on in this post.
Here’s a true story about this.
I was going from hospital to hospital teaching a course in Bioethics (hardly anyone in the health care sector understands what this really is, by the way). I’m in a 30 bed rural hospital, 150 miles from any big city. The subject came up about the money being spent in the USA for health care. Someone brought up doctors’ salaries. A nurse got up and spoke in a thick English accent. These were her exact words, “I would never go back to England and be a nurse, because my salary here is astronomical compared to what I was paid in England.”
Yes, she used the word astronomical!!
OK, you’re getting the picture but this is still sort of my opinion and anecdotes (with references to back it up, though). How about an analysis by some of the top health care economists in the USA? Well, here’s that:
If you don’t know or believe that these guys are the heavy hitter health care economists, just Google Uwe Reinhardt.
Notice the reference to lower use of health services. Yes that’s true, except for those high tech devices you read about in the last post (which aren’t solely driving the difference in total costs per capita).
I could actually go on for dozens of pages with examples of hospitals in “one-hospital” cities and towns charging whatever they want, ancillary service providers employing pricing strategies, endless pharmacy pricing examples, etc. But, now, I’m going to shut up and just show you the data.
Let’s start with some capacity data. According to the Dartmouth Atlas, the more capacity, they higher the utilization of services and the higher the costs. These graphs will show you that, from a global perspective, that isn’t the case because the USA has lower capacity of doctors and hospitals than other countries and the costs are HIGHER. The one thing we are equal with regard to capacity is nurses.
OK, so that Dartmouth Atlas fundamental doesn’t work there! Here’s why: It’s the prices! The Dartmouth Atlas is based on Medicare data with a standardized fee schedule. The prices are fixed.
The Doctors
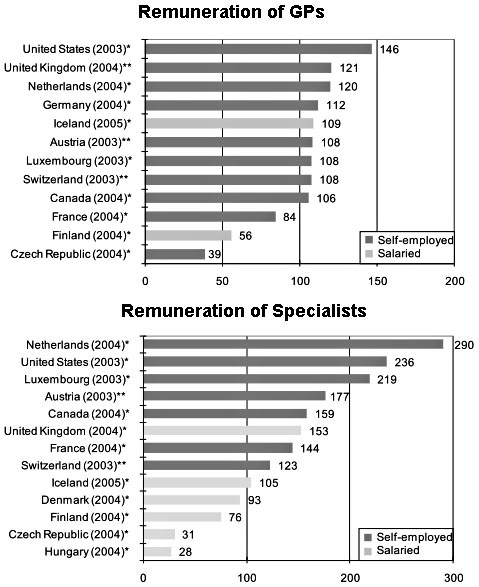
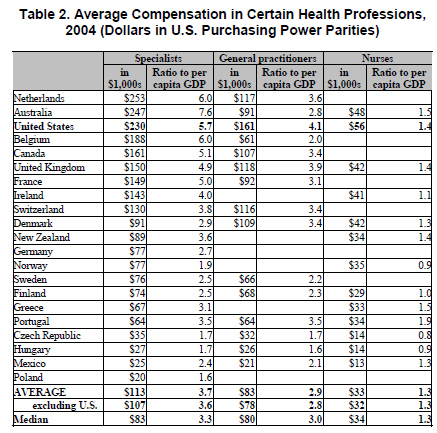
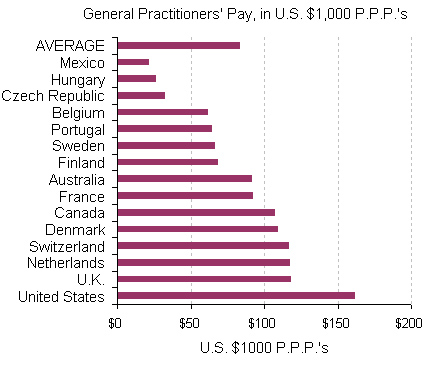
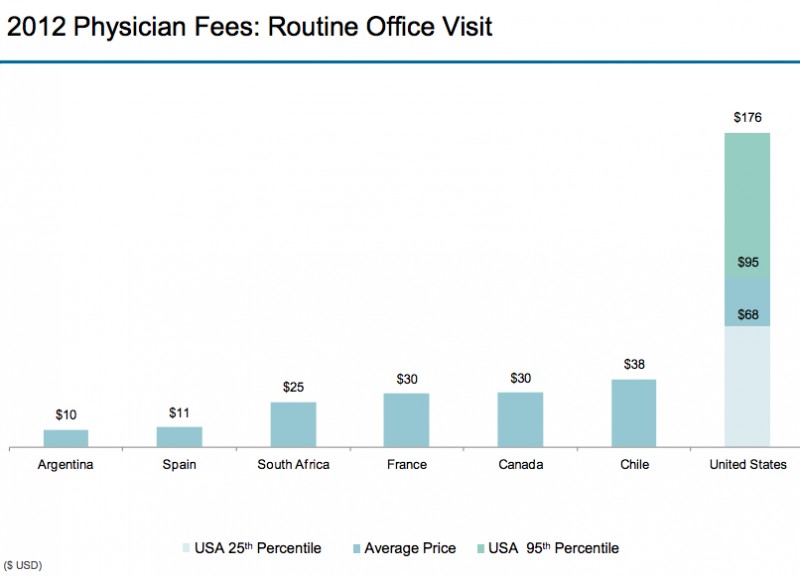
We pay PCPs and nurses more than any other country. Specialists are third. But we have more high cost specialists than any other country. Suggests more referrals from lower cost PCPs to Specialists so the unit cost of physician care is higher.
What about Hospitals?
Less Hospital beds.
Less and declining hospitals.
Shorter Hospital Admissions

Cost per day in the Hospital
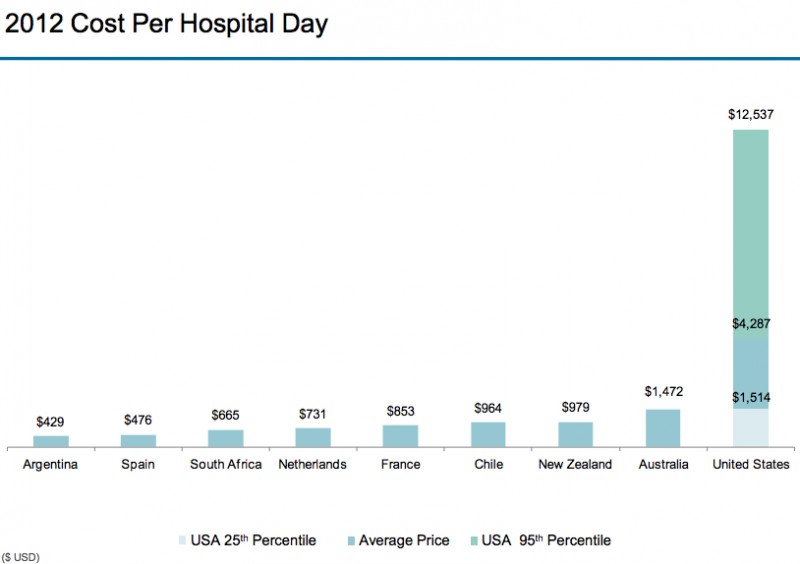
USA has half the hospitals and length of admissions but 4x the average cost of a hospital day. Prices….
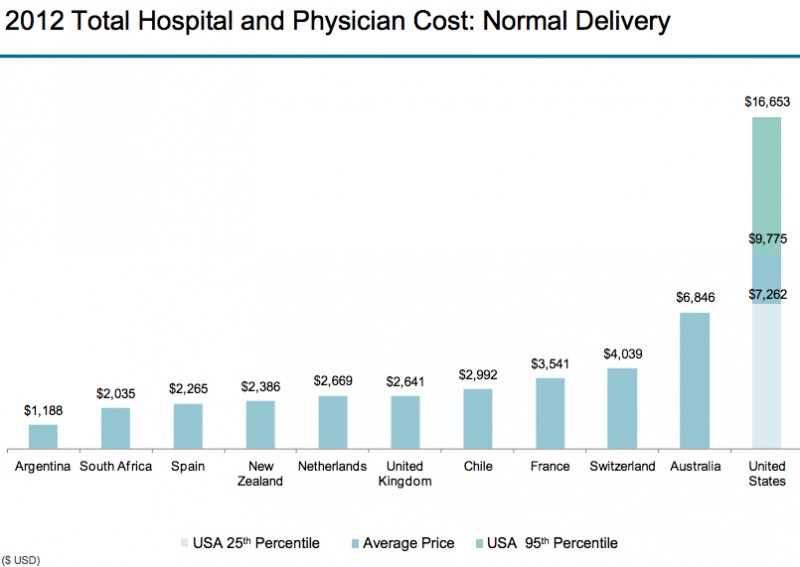
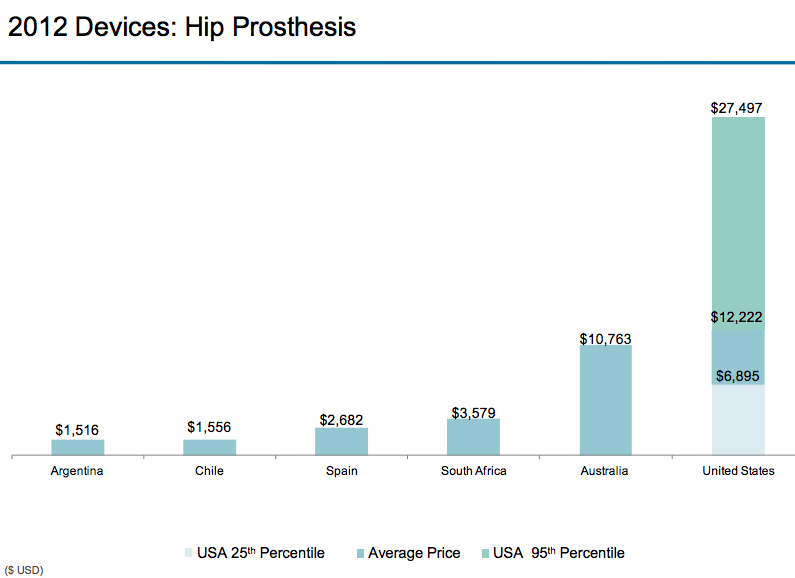
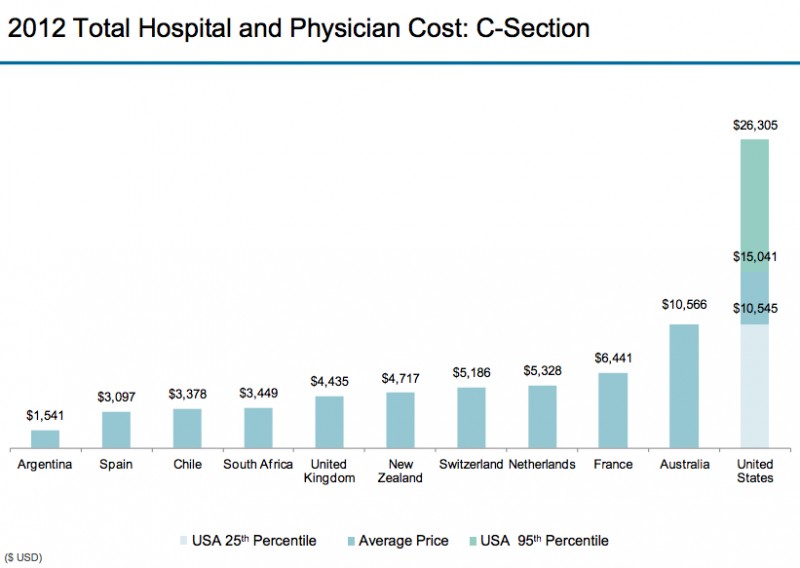
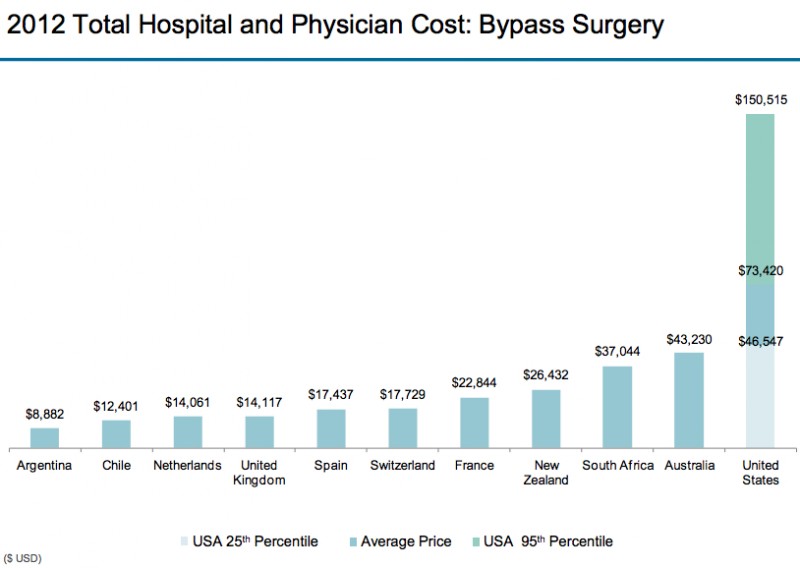
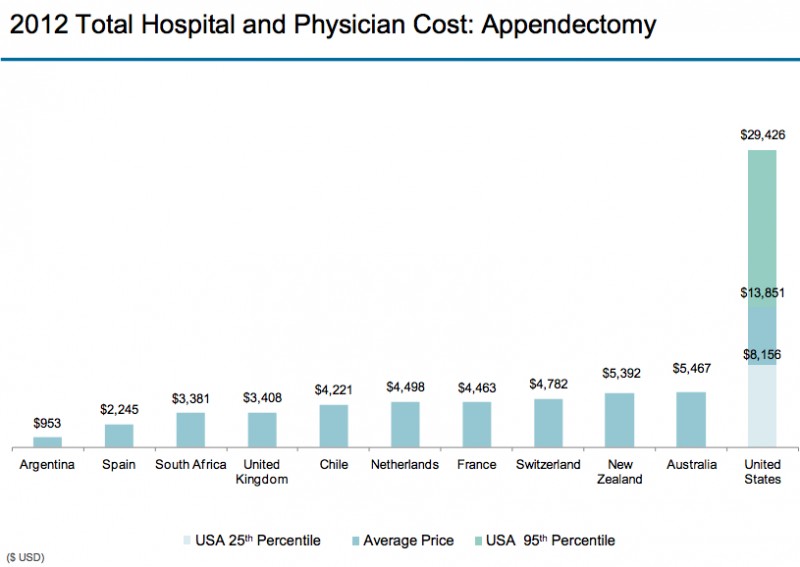
Cost of Hospital Procedures
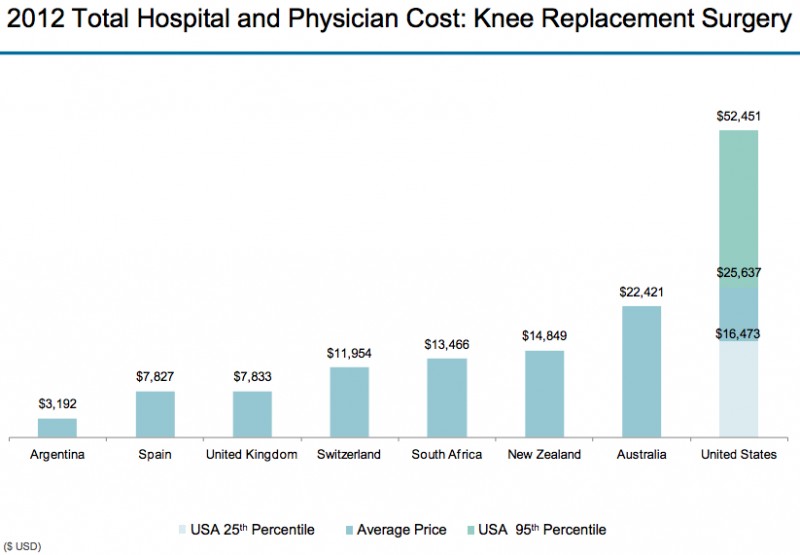
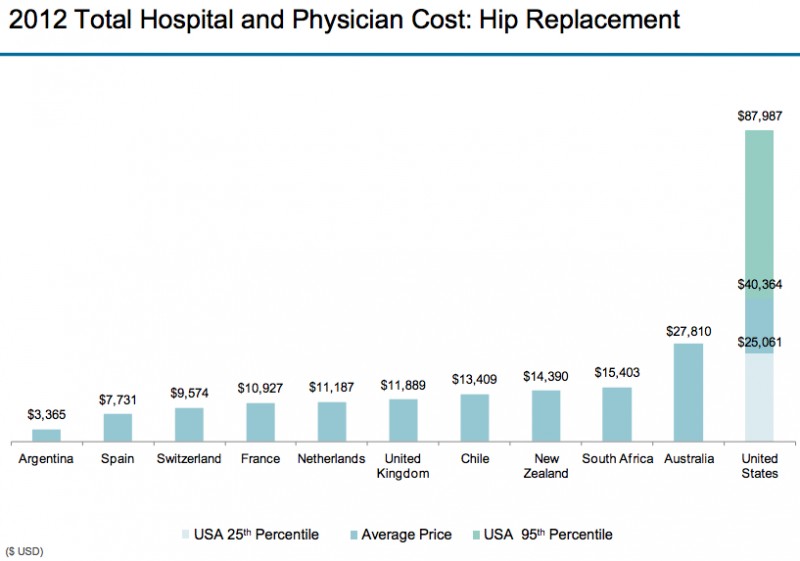
The Prosthesis is the actual artificial hip they put into patients.
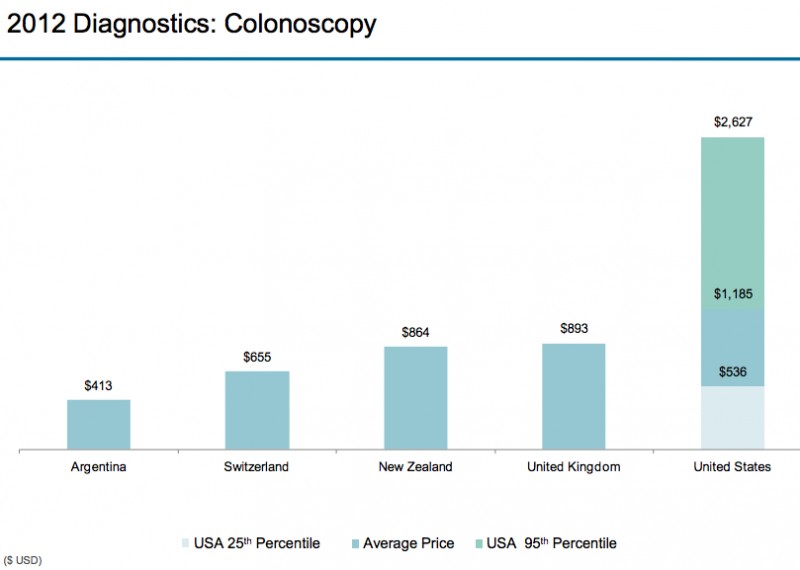
If you’re on a high deductible health plan, want to go to Argentina for your Colonoscopy?
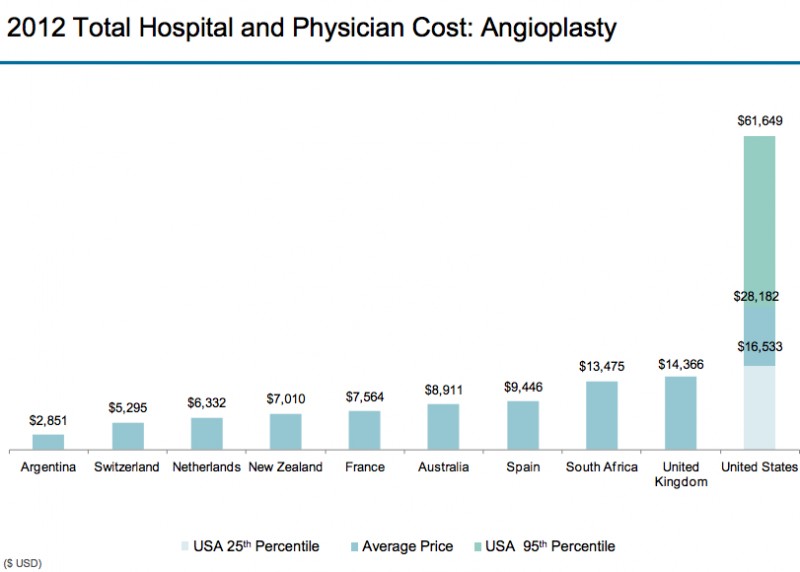
An Angioplasty is what you get to reverse or prevent a heart attack, without having to have surgery.
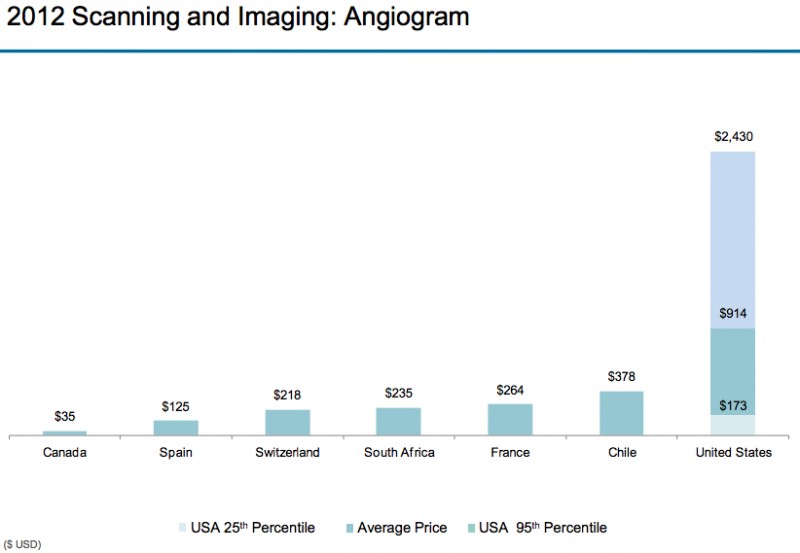
An angiogram is an X-ray where they inject a dye so they can see what your arteries look like.
And then there is the Pharmaceutical Industry
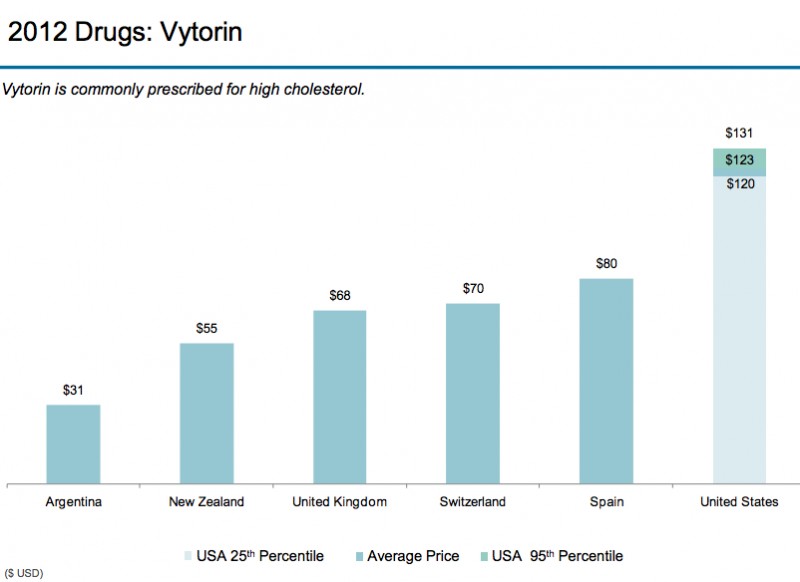
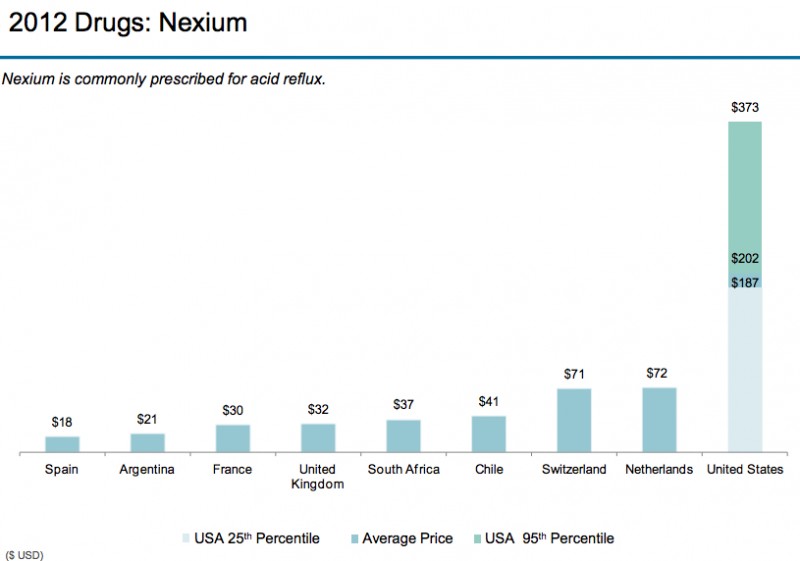
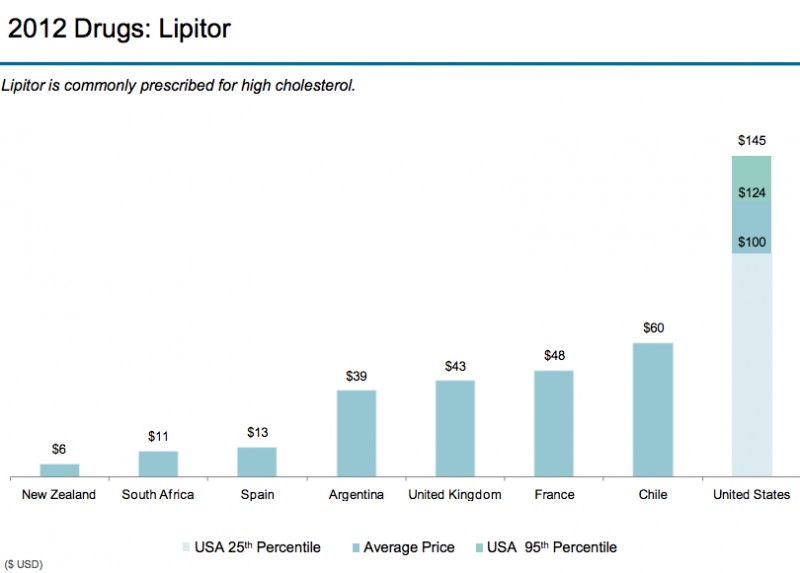
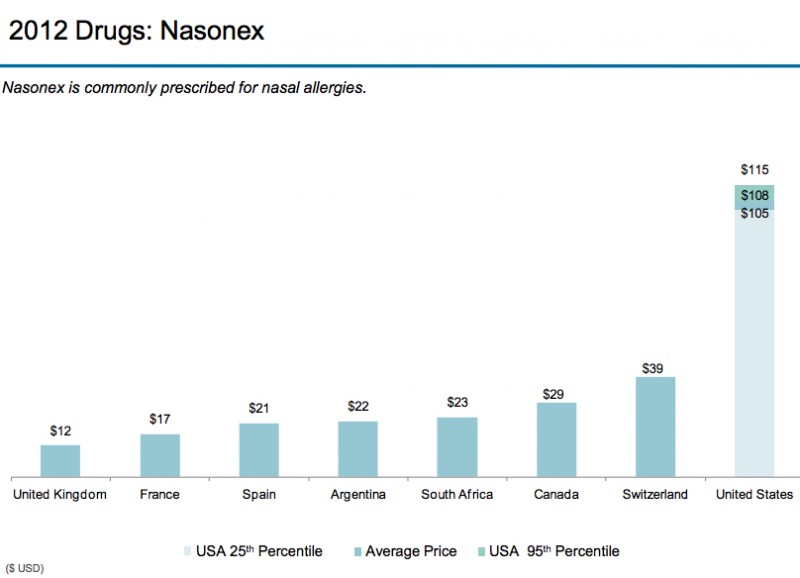
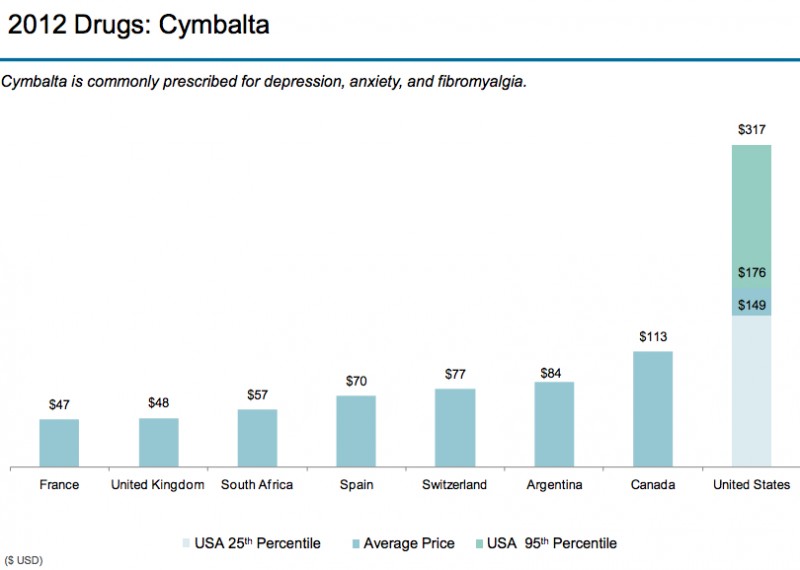
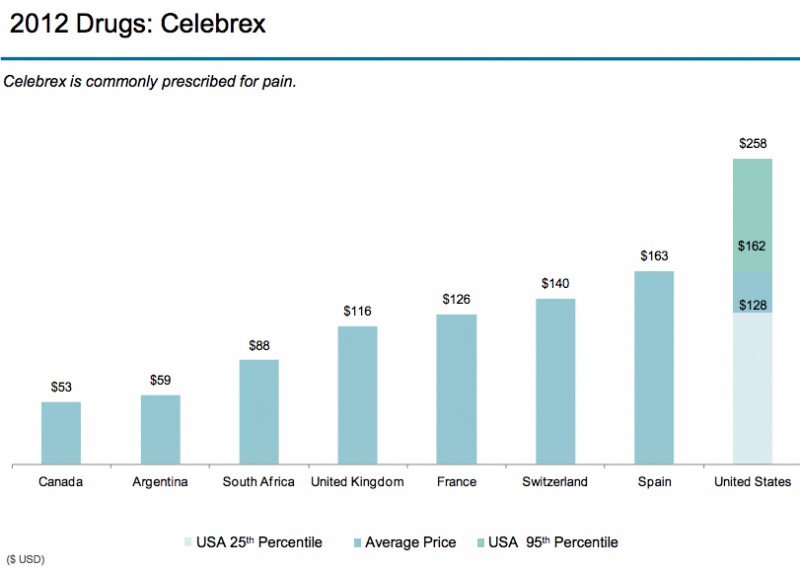
Got the point?
Summary
- The main reason why health care costs are more in the USA than other countries is higher prices.
- The USA has higher prices because the USA is a free enterprise country. It’s perfectly acceptable for a health care provider to charge or negotiate for as much money as they can get.
- Health care providers use a variety of tactics to maximize their revenue/income at the expense of the general pubic/citizens.
- The competition component of the free enterprise system is generally absent in health care economics, which most economists and health care administrators downplay or deny, fueling US health care cost escalation.
[Addendum; The following article was published in the Annals of Family Medicine in their July/August 2017 issue: “Comparing Medical Ecology, Utilization, and Expenditures Between 1996-1997 and 2011-2012”; Ann Fam Med 2017;15:313-321. https://doi.org/10.1370/afm.2084. It documents the same phenomenon as I saw in the fourth paragraph from the beginning of this post, which the finance folks perpetually dismissed:
“Although the number of individuals with visits during an average month and the total utilization of medical services were largely unchanged between the 2 time periods, total expenditures increased markedly. ”
“Over the past 15 years, changes to the medical care system and society at large have resulted in no differences to small differences in most categories of medical care in terms of the number of individuals seeking care or in the number of services. On the other hand, the expenditure framework showed increases in expenditure in nearly every category. Total expenditures increased by 47.2%, from $246 per individual per month in 1996-1997 to $362 per individual per month in 2011-2012. During this same time, the total number of individuals with a visit in an average month and the total number of visits were unchanged. Collectively, the study’s findings therefore suggest that the increases in expenditure have little to do with an increase in the number of individuals receiving services or the total volume of services, but much to do with the cost of treating the same number of individuals with the same number of services.”
It’s the prices, stupid!